Timely post by Olea Kiosks on RHTP — we like kiosks but CMS explicitly frames tech innovation to include improving access to remote care, data sharing, and cybersecurity, etc. The states decide where the money goes and they are given basic guardrails by the Feds.
RHTP (the Rural Health Transformation Program; CMS also calls it the Rural Health Transformation (RHT) Program) is a huge, time-limited funding stream—$50B over FY2026–FY2030, routed through state-led plans to improve access, workforce, technology, and care models.
Is RHTP “making up for shortfalls” in rural healthcare?
Partially at best—and not by itself.
- What it can cover well (short-run):
- Onetime or catalytic investments (telehealth capacity, IT/cybersecurity upgrades, care coordination infrastructure, workforce pipeline programs, regional partnerships). cms.gov
- What it usually can’t “fix” alone (structural, ongoing):
- Chronic operating losses driven by low volume, high fixed standby costs (ER/OB), payer mix, staffing costs, and the fact that rural systems often need permanent payment redesign more than short-term grants.
- A key constraint: it’s temporary (5 years) and depends heavily on how each state designs and targets its plan—so results will vary a lot.
Is rural healthcare “on a path to doom”?
Not doomed—but on a high-risk trajectory without sustained reforms. We see that with our healthcare in Oklahoma. Smaller hospitals squeezed out of operation.
- Why it’s high-risk: rural systems face persistent workforce shortages, limited specialty coverage, and financial fragility; a 5-year program can stabilize and modernize, but it doesn’t automatically create durable revenue and staffing.
- What would indicate it’s not on a doom path (watch these):
- States use RHTP to lock in sustainable access models (shared services/regional networks, right-sized service lines, reliable transfer pathways).
- Workforce retention improves (not just recruitment) and scope-of-practice bottlenecks ease.
- Payment approaches explicitly cover standby capacity (24/7 ED, obstetrics, EMS integration), so essential services aren’t funded like optional volume services.
Because Congress/CMS set RHTP up as a state-led, state-tailored program rather than a single uniform federal operating subsidy.
- Healthcare delivery is local: rural needs differ a lot (frontier vs. small-town, hospital-based vs. clinic-based, OB/EMS gaps, distance to tertiary centers), so states are allowed to target funds where their access failures are worst.
- States control many “levers” that determine success: licensure and scope-of-practice rules, Medicaid policy choices, rate-setting approaches in some states, and how to organize regional networks and workforce programs—so CMS requires a state plan that aligns with those levers.
- Medicaid is inherently a federal–state partnership: lots of rural financing flows through Medicaid, so the program is structured to run through state strategies and implementation rather than bypassing them.
- Accountability and evaluation: the design uses state applications/plans, milestones, and reporting so CMS can compare approaches and adjust over time.
- Net effect: the federal government provides funding + guardrails, while states decide who gets it, for what, and how it’s implemented, which is why outcomes will vary.
Our “Other Side of the Coin” POV
The blogpost is partly accurate on the big picture (RHTP/RHT exists; it’s ~$50B/5 years; states run the subawards; “tech innovation” is a real strategic goal), but the post is not a reliable guide to what will be funded or what qualifies—it’s more of a vendor marketing piece aimed at steering RHT dollars toward kiosks.
Yes—odds are good that most states will put meaningful RHTP/RHT dollars into telehealth/technology-enabled care and cybersecurity/IT modernization, because those uses are explicitly contemplated under the program’s tech-focused goal and “major IT advances” language, and they’re broadly applicable across rural settings.
Caveat: the mix will still vary by state, and states may prioritize “telehealth that fills a clinical access gap” (behavioral health, specialty consults, remote monitoring) over generic video-visit expansion.
Follow the Money Applies?
What mega companies like UHC could realize
- Indirectly (most likely): rural hospitals/clinics use RHT funds to buy services from vendors (telehealth platforms, care management tools, cybersecurity), or to stand up programs that incidentally reduce costs for all payers.
- Directly (possible but uncertain):
- If a state uses RHT funds for payments tied to care delivery through arrangements that include ACOs or similar entities, and UHC-affiliated groups participate. cms.gov
- If a state competitively awards a contract to an Optum/UHC-related vendor for tech, analytics, care coordination, or security services (this is state procurement-dependent, not guaranteed by statute). cms.gov
What’s the best estimate right now?
Unknown / not publicly knowable in aggregate yet. CMS has not published a national breakdown showing how much will flow to specific companies like UnitedHealthcare; you’d have to track state award documents and contracts as they roll out.
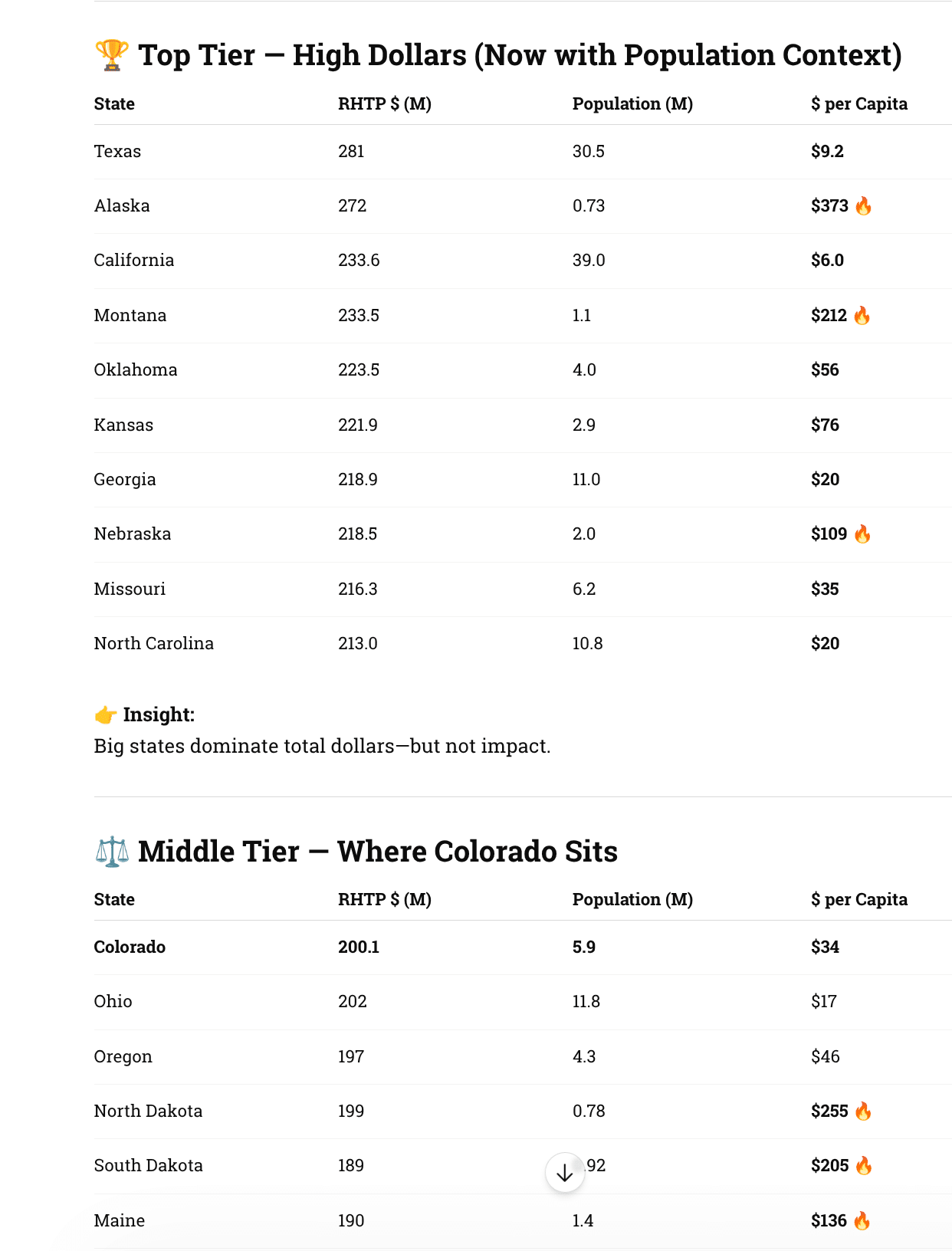
What About Colorado As Example?
- Colorado alone expects ~$200M in initial funding — a real test case for how states deploy RHTP dollars.
- The program covers all 52 rural counties — but allocation decisions remain state-driven.
- Colorado will get meaningful RHTP money — but whether it funds real access solutions or just spreads dollars thin across initiatives is still an open question.
How much Colorado gets (early signal)
- Colorado expected ~$200M in the first year alone
- Funding continues annually through 2026–2030 as part of the national $50B pool
👉 That lines up with our framing: ~$200M/year scale per state (ballpark, not fixed)
🧠 What Colorado is actually targeting
Colorado’s plan is not abstract — it’s pretty aligned with our post:
- Coverage across 52 rural + frontier counties
- Focus areas:
- Telehealth / access expansion
- Workforce shortages
- Behavioral health integration
- IT + system modernization
👉 That directly supports our thesis: telehealth + cybersecurity + infrastructure = likely winners
What About Dispersion Between the States?
California didn’t do to good…
More Data
Best States for Kiosk + Telehealth Deployment (RHTP Era)
🔥 Tier 1 — Prime Targets (High $ + Real Need + Execution Likely)
Texas
- Massive funding + huge rural gaps
- Strong hospital networks + private partners
- Best for scale deployments (QSR-style rollout thinking)
North Carolina
- Proven Medicaid innovation track record
- Telehealth + behavioral health focus
- High probability of structured, repeatable deployments
Georgia
- Rural hospital closures = urgency
- Aggressive modernization stance
- Likely to fund access endpoints (kiosks, remote intake)
Tennessee
- Strong health systems + rural stress
- Known for pragmatic implementation
- Good mix of funding + execution discipline
⚡ Tier 2 — High Impact / High ROI (Smaller States, Big $ per Capita)
Alaska
- Extreme geography → telehealth necessity
- Highest per-capita funding
- Ideal for telehealth kiosks, remote diagnostics
Montana
- Sparse population + high funding density
- State likely to prioritize access infrastructure
- Strong candidate for regional kiosk networks
North Dakota & South Dakota
- Very high $/capita
- Workforce shortages = automation opportunity
- Best ROI per deployment (less competition, more impact)
Nebraska
- High funding + centralized healthcare systems
- Easier statewide coordination
- Quiet but strong execution candidate
⚖️ Tier 3 — “Execution States” (Including Colorado)
Colorado
- Solid funding (~$200M)
- Covers 50+ rural counties
- Outcome depends entirely on state decisions
👉 Your backyard insight:
- Good for pilot programs + partnerships
- Not guaranteed to scale without advocacy
Oregon
- Progressive telehealth policy
- Strong rural/urban divide
- Good for behavioral + access kiosks
Minnesota
- Mature healthcare systems
- Likely to invest in coordinated care tech
- Less flashy, more structured deployments
📉 Tier 4 — Lower Priority (For Now)
California
- Huge dollars, but diluted impact
- Complex procurement + bureaucracy
- Hard to penetrate despite size
New York
- Similar story: big money, slow execution
- Focus on system-level reform vs endpoints
New Jersey, Massachusetts
- Low rural need
- Lower RHTP relevance
- Less demand for kiosk/telehealth infrastructure
🧠 What Actually Drives “Best State”
🎯 1. Funding Density (not total dollars)
- Dakotas > Texas (per deployment ROI)
🏥 2. Rural Access Gaps
- More gaps = more justification for kiosks/telehealth
⚙️ 3. State Execution Culture
-
North Carolina > California (in practice)
🤝 4. Procurement Reality
-
Some states fund pilots
- Others fund deployments
The best states for kiosk and telehealth aren’t the ones with the most money —
they’re the ones with the most pressure to solve access problems and the ability to execute quickly.