AI Assisted Healthcare
From KioskIndustry —
While it’s hard not to roll your eyes at voice assistants getting added to every single thing in the smart home, a Los Angeles hospital is actually putting Amazon Alexa to good use. About 100 patient rooms at Cedars-Sinai will now be equipped with Amazon Echos to help patients and caregivers interact more efficiently.
Editors Note: Originally published on Gizmodo 2/26/2019. This is an excerpt.
The pilot program runs off an Alexa-powered platform called Aiva. Now, patients can easily say things like, “Alexa, change the channel” or “Alexa, tell my nurse I need to use the restroom.” Some requests, like turning a TV on or off, Alexa can handle on its own. Others will be sent directly to a caregiver’s cellphone. And, probably the most helpful feature for healthcare providers is that the Aiva platform will be able to send requests to the appropriate type of caregiver. So while a nurse would get any requests for painkillers, a clinical partner would get bathroom requests. According to Cedars-Sinai, requests that take a while to fulfill would then get bumped up the chain of command.
Read Full Article
Excerpt:
While this might raise concerns about automation stealing jobs from qualified healthcare professionals, I’d argue it actually does the opposite. It does play into automation’s narrative of efficiency, but you’re essentially helping out overworked nurses at already understaffed hospitals. Arguably, if you’re a qualified nurse, the last thing you want to spend your time doing is changing TV channels when a patient elsewhere might be in need of painkillers. Plus, there’s just no way Alexa’s ever going to be able to take your blood samples even if you ask it nicely.
More articles
https://kioskindustry.org//now-available-just-ask-alexa-whats-new-at-redbox/
https://kioskindustry.org//amazon-said-to-plan-premium-alexa-speaker-with-large-screen/
https://kioskindustry.org//kroger-launches-voice-assistant-ordering-for-grocery-ecommerce/
Alexa Use in Hospitals (2025)
The use of Alexa in hospitals has increased notably over the last few years, and its presence in patient rooms is becoming more common. Hospitals often use Alexa Smart Properties, Amazon’s healthcare-focused platform, to enhance patient experience and operational efficiency. Notable systems like BayCare Health and Cedars-Sinai have rolled out Alexa devices in hundreds of patient rooms, allowing patients to control their environment (lights, TV, call nurse, entertainment, etc.) and communicate easily with care teams—all hands-free. Hospitals have found that voice assistants are intuitive for patients regardless of age or technical experience and are a “game-changer” for engagement and workflow.nurse+2
-
BayCare Health System (Florida): As of 2025, Alexa is installed in all 16 hospitals in the system, offering patients control over room amenities and streamlining entertainment and communication with staff. Some patients even expect Alexa devices in their rooms, highlighting growing adoption and familiarity.mobihealthnews
-
Patient Experience: Hospitals report improved patient satisfaction and more efficient workflows due to voice assistant integration.healthcareweekly
AI Assistant Trends in Hospitals
Use of other AI assistants (including voice AI and virtual medical assistants) has also increased—dramatically.
-
Widespread Adoption: As of 2025, over 80% of U.S. hospitals use some form of AI assistant to improve patient care and operational efficiency, whether through voice, chat, or workflow automation.litslink+1
-
Market Growth: The virtual medical assistants market was valued at $1.41B in 2025, with annual growth rates around 30% and further rapid expansion expected. Nearly half of healthcare organizations use or plan to implement AI-powered virtual assistants, with common applications including appointment scheduling, routine patient queries, triage, prescription refills, and patient education.golean+1
-
Voice AI in Call Centers and Patient Communication: Hospitals like Houston Methodist have used AI voice assistants to handle massive patient call volumes—especially during health events like vaccine rollouts—automating up to 91% of inquiries and dramatically reducing costs by minimizing human staffing needs.simbo
-
Automated Intake, Triage, Decision Support: Beyond patient rooms, AI assistants power administrative workflows (e.g., admissions, billing), handle documentation, and support clinicians using large language models for diagnosis and protocol recommendations.ishir+2
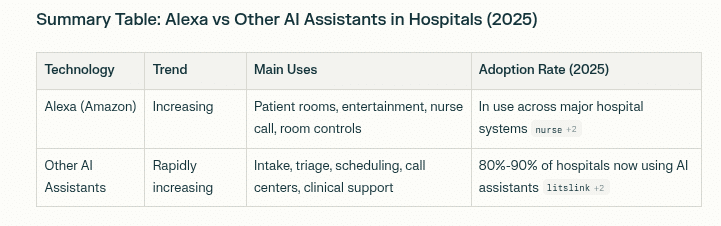
Summary: Alexa vs Other AI Assistants in Hospitals (2025)
alexa adoption rate hospitals
Insights
-
Alexa use is clearly rising in U.S. hospitals—driven by patient and staff demand for intuitive, hands-free interactions.
-
AI assistant adoption as a whole has surged, with nearly every hospital deploying either voice or virtual agents for both clinical and administrative tasks.
-
Voice AI agents are expected to become universal, with benefits for patient satisfaction, cost efficiency, and operational scalability.hyro+1
In summary, both Alexa and other AI assistants are being used much more widely in hospitals in 2025 compared to prior years, with the trend strongly upward for both categories.